Every expecting parent hopes for their child to be born healthy. Genetic testing of embryos may detect possible problems early on and ensure that only healthy embryos are transferred.
Genetic abnormalities are the most prevalent reason for repeat first trimester miscarriages. With PGD the success rate of live births is proven to have greatly increased.
In Europe, unfortunately, PGD is not open to all parents. In Switzerland the laws have been slightly relaxed so that at least couples with a medical history of miscarriages and high risk of complications may take advantage of testing. For everyone else wanting to undergo preventive tests however, PGD is prohibited.
Only few countries have less restrictive legal parameters, but there, carefully selected IVF clinics offer the highest success rates.
Difference between PGD and PGS (PGT-M and PGT-A)
Preimplantation Genetic Diagnosis or PGD (PGT-M) is recommended when one or both parents suffer from a known genetic disorder or carry a genetic predisposition with a high probability it may be passed on to their child. PGD allows doctors to focus specifically on chromosomal defects. Only embryos without faulty genes are transferred to the womb.
Preimplantation Genetic Screening or PGS (PGT-A) is helpful for healthy partners as a preventive measure to screen for potential genetic abnormalities. Especially those who have undergone one or multiple unsuccessful IVF treatments without pregnancy. In some countries like Northern Cyprus and Ukraine, specialists also use PGS to identify X or Y chromosomes, making this method most reliable in determining the embryo’s gender.
PGS and Genetic Conditions
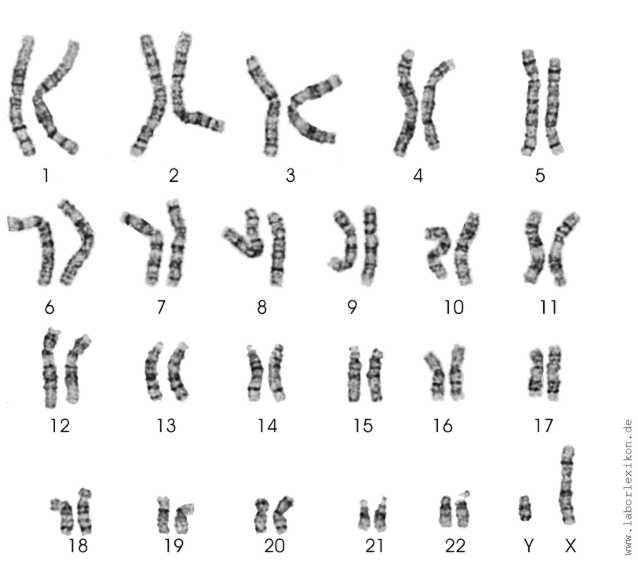
With PGS, testing is done to detect chromosomal defects responsible for genetic conditions such as Down syndrome (trisomy 21), Edwards syndrome (trisomy 18), Patau syndrome (trisomy 13), Turner syndrome (monosomy X) and Klinefelter syndrome (trisomy XXY).
PGD and PGS in the Laboratory
After a waiting period of 72 hours post fertilization of the harvested egg, the embryo now consists of enough cells for testing. In the laboratory one or more cells are removed and analyzed. The embryo is not harmed by this procedure and continues to develop normally.
Within 48 hours test results are available and after consulting with the geneticist the doctor is able to properly advise the patient on making an informed decision.
However, PGD cannot detect all chromosomal defects. Some disorders express themselves in so called mosaic embryos, consisting of a mix of two or more different genetic constitutions. Anomalies can only be traced in a certain percentage of cells. PGD with examination of just the right cells is crucial for detection. Also, there are some very rare disorders that are not commonly tested for. A list of all possible analyses is available through our doctors.
PGD is not a substitute for PGS. With PGD only genetic disorders already manifest in the family are checked for. Down syndrome for example, would only be detected with PGS.

«PGD can increase the success rate of having a healthy baby by over 50%.»
When do Doctors recommend PGD and PGS?
- Repeat miscarriages
- Multiple unsuccessful IVF cycles
- Previous live or stillbirth of a baby with chromosomal anomaly
- Age related risks (mothers over 36 years old)
- Prevalence of a sex related disorder in the family with consequent gender selection of embryo.
- Use of surgically harvested sperm (MESA/TESE).
- One of the parents is carrier of a genetic mutation.
- Prevalence of one of the following commonly identified genetic diseases: Cystic fibrosis, Fragile X syndrome, Hemophilia, Thalassemia, Sickle cell anemia, Phenylketonuria, Mutation of tumor suppressing gen.
- IVF resulting in only a small number of embryos.
Findings by International Specialists
At the beginning of the 1990s, UK Professor Alan Handyside played a major role in the development of the PGD method and its introduction to clinical practice. The first recorded pregnancy with PGD in Central Europe was in the Czech Republic in 2001.
On the occasion of the 25th anniversary of the introduction of PGD, Professor Handyside summarized his experiences so far. According to his research, PGD can increase the success rate of having a healthy baby by over 50%.